


Caffeine’s impact and neurochemical pathways in neurotypical, ADHD, and autistic brains



An extremely simplistic version of the detailed synthesis below (image generated by ChatGPT).
International coffee organization estimates that around 1 billion of the world population regularly drinks coffee. The National coffee association estimated that 66% of US adults drink coffee regularly. Tea is consumed in every country worldwide and 40% of the world population are estimated to be tea drinkers. Caffeine is present in both these beverages – therefore, a naturally occurring bioactive compound found in coffee, tea, cocoa, and other plants. The psychoactive property of caffeine is valued for its ability to sharpen alertness and ward off drowsiness.
However, the effects of caffeine are found to vary in neurodivergent people (Autism Spectrum Disorder, ADHD, dyslexia, Dyspraxia / DCD, Tourette Syndrome, neurodevelopment component of epilepsy, Intellectual Disability, Bipolar Disorder, Schizophrenia and other sensory processing differences) as compared to neurotypical individuals. This difference may be attributed to distinct neurochemical balances in neurodivergent individuals based on the type of neurodivergent condition. Thus, caffeine’s mechanism of action and neurochemical pathways play out differently in neurodivergent individuals.
Neurotypical Brain and Caffeine- Adenosine antagonism and arousal
In a neurotypical brain, caffeine increases wakefulness and alertness and this stems from its action as a non-selective adenosine receptor antagonist. This means that when a person is awake and using up ATP or energy molecules, the byproduct which is a neuromodulator adenosine accumulates in the brain. This adenosine binds to its receptors (A₁ and A₂A subtypes) which then leads to neuronal inhibition and drowsiness.
When adenosine docks on A₁ receptors widespread in the brain, it typically suppresses neural firing and the release of excitatory neurotransmitters, promoting sleep and reducing arousal. Binding of adenosine to A₂A receptors (highly expressed in regions like the striatum) can dampen dopamine signaling, because A₂A receptors form functional complexes with dopamine D₂ receptors in those neurons. In essence, adenosine is a physiological brake on brain activity and alertness.
Caffeine is chemically a methylxanthine and structurally similar to adenosine, allowing it to fit into adenosine receptors without activating them. By occupying adenosine’s binding sites, caffeine prevents adenosine from exerting its effects and the immediate consequence is the blunting of inhibitory, depressant influence of adenosine and the neurons that would normally be muffled by adenosine, will remain active, and in some cases even increase their firing.
When caffeine blocks A₂A receptors in the basal ganglia, it lifts the suppression on dopamine signaling, effectively enhancing dopamine’s action on D₂ receptors. This mechanism helps explain caffeine’s mild euphoriant and psychostimulant properties.
In parallel, caffeine’s adenosine blockade leads to elevated release of other neurotransmitters like norepinephrine and acetylcholine, further contributing to arousal and increased neuronal excitability. The net effect is that a typical dose of caffeine causes a person to feel more awake, vigilant, and able to concentrate, therefore, countering fatigue.
Caffeine’s actions are dose-dependent and not entirely limited to adenosine receptors. At higher concentrations, caffeine has other biochemical effects such as phosphodiesterase inhibition leading to increased cyclic AMP, calcium mobilization, or even weak antagonism of GABA_A receptors.
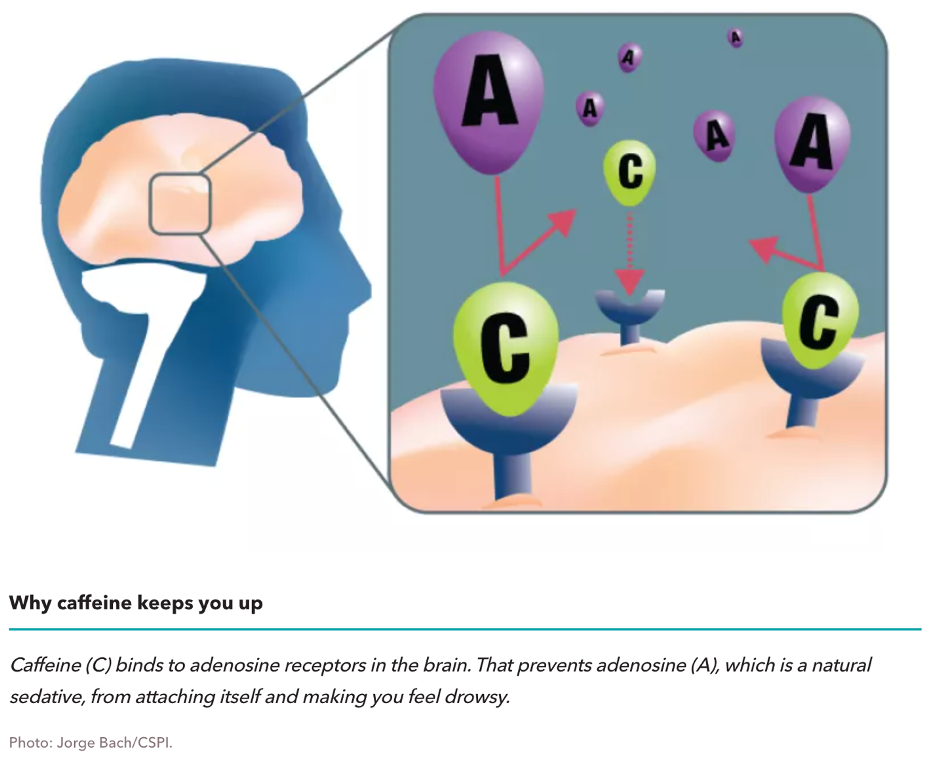
From: https://www.cspinet.org/article/caffeine-helping-or-harming-your-health
ADHD Brain and Caffeine- dopaminergic modulation and stimulant parallels
ADHD is a neurodevelopmental condition classically associated with dysregulation of catecholamine neurotransmitters, especially dopamine and norepinephrine, in fronto-striatal circuits. The core symptoms of ADHD like inattention and impulsivity are linked to underactivity of these neurotransmitter systems in the prefrontal cortex. This is why first-line ADHD medications are stimulants that increase synaptic dopamine and norepinephrine, leading to improved focus and self-control. Intriguingly, caffeine – a far milder psychostimulant – acts on some overlapping pathways, raising the question of whether it can be therapeutic.
In an ADHD brain, which is dopamine deficient, this adenosine antagonism by caffeine might help boost dopamine’s effects, similar to methylphenidate or amphetamine improving attention by elevating dopamine-norepinephrine levels. Caffeine might improve alertness and concentration in ADHD by preventing adenosine from stifling dopamine and by raising norepinephrine release.
In the spontaneously hypertensive rat, a well-validated animal model of ADHD, caffeine treatment has been shown to normalize certain dopaminergic functions and improve cognitive performance. In this study, chronic caffeine administration in spontaneously hypertensive rat improved memory and attention measures, aligning with the concept that enhanced dopamine signaling was beneficial.
ADHD may also involve adenosine system differences. Some genetic evidence points to the adenosine A₂A receptor gene (ADORA2A) to be nominally associated with ADHD traits. Moreover, an interaction between A₂A receptor gene variants and dopamine D₂ receptor gene variants has been linked to a higher risk of anxiety in children with ADHD. This suggests that the adenosine-dopamine interplay, providing a mechanistic rationale for why an adenosine antagonist like caffeine might modulate ADHD symptoms.
Many ADHD individuals self-medicate with caffeine (in the form of coffee, energy drinks, etc.) to help their concentration. However, the clinical evidence for caffeine’s effectiveness in treating ADHD is mixed and overall, not strongly favorable. A recent systematic review and meta-analysis (2023) of randomized controlled trials in children with ADHD concluded that caffeine did not produce significant improvement in core symptoms compared to placebo. In that analysis, which pooled data from several small trials, the overall effect of caffeine on ADHD symptoms was statistically no different than placebo (with a tiny effect size in favor of caffeine that was not significant). Qualitative analysis of the studies showed minor benefits where one trial noted improved sustained attention with paradoxical worsening of impulsivity with caffeine, while another found a modest improvement. Four studies found no meaningful improvement in inattention or hyperactivity relative to placebo. These findings underscore that caffeine’s pro-alertness effect, while real, is generally too small and inconsistent to rival the targeted impact of pharmaceutical stimulants for ADHD.
There are several factors might explain caffeine’s limited efficacy in ADHD.
1. Dose- a higher dose of caffeine might be needed to significantly affect dopamine/NE in the ADHD brain, but those doses carry side effects (jitters, anxiety, insomnia) that offset benefits.
2. Tolerance: regular caffeine use leads the brain to upregulate adenosine receptors as an adaptation, diminishing its stimulant effect over time. Interestingly, epidemiological observations show that adolescents with hyperactivity tend to consume more caffeine than their peers, perhaps seeking relief, but resulting in worse symptoms due to high doses of caffeine and yet still not achieving full symptom control.
Therefore, while caffeine shares a mechanistic overlap with ADHD medications by boosting dopaminergic and noradrenergic activity indirectly, and it can produce mild improvements in attention or cognition. In real life, this may not be a reliable or potent solution similar to ADHD stimulants. Current studies reveal that while caffeine has some pro-cognitive effects in ADHD models, it falls short as a clinically recommended treatment for children.
Autistic brain and caffeine- excitation–inhibition balance and adenosine signaling
Autism Spectrum Disorder or autism is neurochemically distinct from ADHD. One is that many autistic brains exhibit an imbalance between excitatory and inhibitory signaling or E/I imbalance, with excess excitation or insufficient inhibition in neural circuits. This E/I imbalance contributes to sensory overload, hyperactivity, seizures etc.
Adenosine is a neuromodulator that generally promotes inhibition, and any alteration in adenosine signaling in autism could shift the E/I imbalance. Researchers have investigated adenosine in the context of ASD and found that the adenosine A₂A receptor (A₂AAR) implicated in autism.
Genetic studies have found that certain variants of the A₂AAR gene (ADORA2A) are more frequent in autism, even related to increased autistic symptom severity and anxiety levels. This indicates that adenosine A₂A receptor function may be somewhat divergent in ASD. A₂A receptors are abundant in the striatum and other dopamine-rich areas, where they influence dopamine and glutamate neurotransmission.
Intriguingly, one of the earliest pharmacological clues came from animal research: using drugs that affect adenosine receptors changed autism-like behaviors. An animal study activating A₂A receptors with an agonist (CGS 21680) was found to attenuate repetitive, stereotyped behaviors in rodents, whereas blocking A₂A receptors (DMPX an antagonist) potentiated those repetitive behaviors.
The consistency of these findings suggests that adenosine signaling is generally protective or modulatory in a beneficial way in ASD models and removing that signaling by caffeine can aggravate core features. It appears that boosting adenosine’s action through receptor agonists or by increasing adenosine levels tends to rebalance neural circuits in a way that reduces autism-like symptoms in animals.
Early clinical investigations align with this picture. In a pilot randomized trial, propentofylline, a compound that blocks adenosine reuptake and also inhibits phosphodiesterase, effectively increasing extracellular adenosine availability – was added to the treatment regimen of children with autism (who were on the antipsychotic risperidone). The children who received propentofylline showed better improvements on the Childhood Autism Rating Scale than those who received placebo. By elevating adenosine levels, propentofylline likely enhanced activation of adenosine receptors, which could contribute to reduced irritability or improved social behavior.
Caffeine being an antagonist of adenosine receptors, we expect to decrease adenosine activity. Thus, theoretically, caffeine could worsen the E/I imbalance in an autistic brain. It might also interfere with the neuromodulatory balance that affects repetitive behaviors or social communication. However, the actual responses of autistic individuals to caffeine are highly variable. Some autistic adults report that caffeine helps them focus or lifts brain fog, while others experience amplified anxiety, jitteriness, or sensory overload from even small amounts of caffeine. This variability likely reflects underlying differences in neurochemistry. One participant’s anecdote can differ wildly from another’s. Thus, no blanket statement can be made that “caffeine helps autism” or “caffeine is bad for autism”. At best, the response to caffeine is idiosyncratic. Therefore, there is a need for further research to fully understand caffeine’s impact on the autistic brain.
What studies reveal and what are the gaps?
1. Research into caffeine’s neurochemical interaction with neurodivergent conditions is still evolving.
2. In ADHD, we have relatively more data: animal studies overwhelmingly show that caffeine can improve attention and hyperactivity measures (e.g. in rodent models) by modulating dopamine and other neurotransmitters, but human trials in children with ADHD have not borne out a clear benefit over placebo.
a. This suggests a gap between preclinical promise and clinical reality, potentially due to dosing issues, tolerance, or simply that caffeine’s magnitude of effect is too small in the context of ADHD.
b. There is a lack of studies in adult ADHD. Most trials focused on children, leaving open the question of whether adults with ADHD might derive more subjective benefit from caffeine (anecdotal) or whether certain subtypes of ADHD respond differently.
3. In autism, the research gap is even larger.
a. The role of caffeine in ASD has not been the focus of many clinical studies.
b. What we know about adenosine in autism comes largely from indirect evidence. These collectively indicate that enhancing adenosine signaling tends to be beneficial for autism outcomes, whereas inhibiting it can be detrimental. We also see that some individuals with ASD respond positively to caffeine on certain measures.
c. There are several unanswered questions for ASD:
i. Are there identifiable genetic or neurochemical predictors for whether an autistic person will respond well or poorly to caffeine?
ii. How does chronic caffeine consumption (not based on dosing) affect autistic adults in terms of anxiety, attention, and sensory processing?
d. Another gap is understanding the long-term neurochemical adaptations in neurodivergent individuals who habitually use caffeine. Neurotypical brains adjust to daily caffeine by increasing the number of adenosine receptors called homeostatic upregulation. If the same happens in ADHD or ASD brains, could that chronic adaptation actually move their neurochemistry toward a more “normal” state since more adenosine receptors could counteract an existing deficit in inhibitory signaling? This is speculative and has not been empirically tested in autism.
e. Additionally, what is the interaction of caffeine with common ASD medications or therapies? Would caffeine synergize with ADHD medications in those with dual diagnoses, or interfere with anxiolytic medications used in ASD?
f. Another gap is in understanding caffeine’s effect on the excitation/inhibition (E/I) ratio in autistic brains in vivo. Does a dose of caffeine measurably increase cortical excitability more in ASD individuals than in neurotypicals? Advanced neuroimaging or electrophysiological studies could answer this, but few have been done.
g. We lack data on whether caffeine influences autism symptoms like social communication in any consistent way? The anecdotes and tiny studies are intriguing but not definitive. Current studies give us mechanistic clues and some initial clinical observations, but there is much uncharted territory. This is especially true for autism, where caffeine’s role is complex and under-investigated, making it a ripe area for further inquiry.
Future directions for research
Given the converging evidence that increasing adenosine receptor activation can ease certain autism-related behaviors
development and testing of drugs other than caffeine that more selectively modulate these receptors, blocks all adenosine receptors acutely, like A₂A receptor agonists or positive allosteric modulators. See if they produce benefits in social behavior, repetitive behaviors, or neural connectivity in ASD.
Clinical trials in humans - to translate early animal studies using A₁ or A₂A agonists. This should be to achieve the desired central effects without side effects like cardiovascular changes
Some researchers have speculated that caffeine could be harnessed therapeutically such as using caffeine or other antagonists long-term to make the brain more responsive to adenosine when the antagonist is removed. In the context of autism, one could hypothesize a regimen where caffeine is used in a controlled manner to induce receptor upregulation, and then withdrawn to allow a surge of adenosine activity that might temporarily improve symptoms. This concept would need careful study. This will be experimentally unorthodox and might not be practical.
Focus on identifying genetic markers like ADORA2A SNPs, levels of adenosine metabolites, EEG signatures of E/I ratio, etc. that predict an individual’s response to adenosine antagonists or agonists.
Adenosine is a neuromodulator and influences neuroinflammation and metabolism. The A₂A receptor also has anti-inflammatory roles in the brain’s immune cells (microglia).
Could some of autism’s pathology be alleviated by targeting neuroinflammation via the adenosine pathway? Whether interventions like caffeine which affects cytokine profiles through A₂A receptors or selective A₂A drugs alter neuroinflammatory markers in ASD and whether that correlates with behavioral changes. Many autistic individuals have co-occurring gastrointestinal or metabolic disturbances, and adenosine is linked to energy metabolism. So, investigating how caffeine affects metabolic and gut-brain signals in ASD could be discerning.
In conclusion, caffeine’s primary trick, which is blocking adenosine’s sleepy signal, interacts with each brain type in unique ways:
the neurotypical brain experiences straightforward stimulation,
the ADHD brain sees a partial dopamine-mediated pick-up (though not as much as dedicated stimulants), and
the autistic brain may be pushed towards either improvement or imbalance, depending on individual neural context.
Future research focusing on adenosine receptor modulation holds some promise for unlocking new strategies to support neurodivergent individuals.
Thank you for sharing this! It seems difficult enough to parse out individually, but I am also curious about impacts in AuDHD folks.
There are many ADHDers - like myself - who find that coffee, whilst often helping with focus, can also make us feel sleepy.